Any physician may submit a question regarding a thyroid patient to ldegroot@earthlink.net and one of our panel of expert thyroidologists will attempt to provide an answer as soon as possible by return Email. Physicians should provide adequate clinical information about the problem, and provide their name, office address, and telephone number. We will send an answer by Email to the address provided, and will publish the question and the response on this page. The name of the questioning physician WILL be published unless specific instruction not to do so is provided in the original Email. This service is available only to physicians.
Please note that Thyroidologists who hold opinions that differ from the advice we have offered are welcome to send in responses, and we will publish these comments. Commentators should kindly include name, office address, and Email address.
We attempt to answer important questions from readers, if time permits, and publish those of value to other readers in this column. Please send questions to Dr John Lazarus lazarus@cardiff.ac.uk
To read questions from patients click here.
MANAGING NIFTP - ENCAPSULATED NODULE WIIH NUCLEAR FEATURES COMPATIBLE WITH PAPILLARY THYROID CANCER BUT LACKING CAPSULE INVASION.
QUESTION--I recently sent a patient for total thyroidectomy for multinodular toxic goiter. Histopath reported "consider NIFTP." Specimen sent for HBMEI, & result is positive . I've read literatures , not recommending RAI for this is reclassified as benign with some Reservations / caveat as " more research is needed for long term medical implications ". What is your recommendation. Thank you always . Lynn Bilar ,MD
RESPONSE-Dear Dr. Bilar, the term NIFTP applies to a totally encapsulated nodule wth nuclear features compatible with papillary thyroid cancer but lacking capsule infiltration and vessel invasion. The decision to change this category into a benign one, is derived from a consensus of experts who not only reviewd the pathological specimens but also reviewed the outcome of the patients. In no case did the authors detect recurrent disease, confirming that the behaviour of such nudules is entirely benign. You can follow your patient without radioiodine, on suppressive therapy. All that is needed is just a neck ultrasound periodically ( every one-two years). I hope this information may be valuable to you, Furio Pacini MD
15 YR OLD MALE WITH WITH PAPILLARY CANCER AND LYMPN NODE METASTASES-- 28 September 2016
QUESTION--Can you please help us with this case of a 15 y/o Male. He also has RHD.
In 2015 he was managed as toxic MNgoiter. Nov 2015: fnab thyroiditis
August 2016: underwent total thyroidectomy +Neck dissection. Histopath: pap ca 2 cm greatest diameter R & isthmus. Extrathyroidal & capsular invasion present, lymphovascular invasion present . LN Level 2,3,4 6/9 + for tumor involvement. LN Level 2b,left 1/1 positive . LN level 6 right , I/1 positive
Pediatric stage: T3N1b
Whole body scan ( sept 1, 2016 residual tracer avid remnants in the anterior neck. No evidence of distant tracer avid mets. TG ab 7.49 1u/ml. TG > 500 ng/ ml.
We're scheduling him for Rai. Sir Is there an existing RAI-131 dosing guide in pediatric patients .
Thanks very much for your inputs. Dr Lynn Bilar
RESPONSE-- I agree with the decision to treat with radioiodine. Regarding the dose in pediatric patients, we usually advocate the use of 1 mCi per kg body weight, but a 15 y/o boy is almost like an adult and thus, in the presence of diffuse lymph node metastases, a fixed dose of 100 mCi (possibly after preparation with recombinant human TSH) should be preferred. Furio Pacini MD
TREATMENT OF ASYMPTOMATIC NODULAR GOITER-22 JUNE 2016
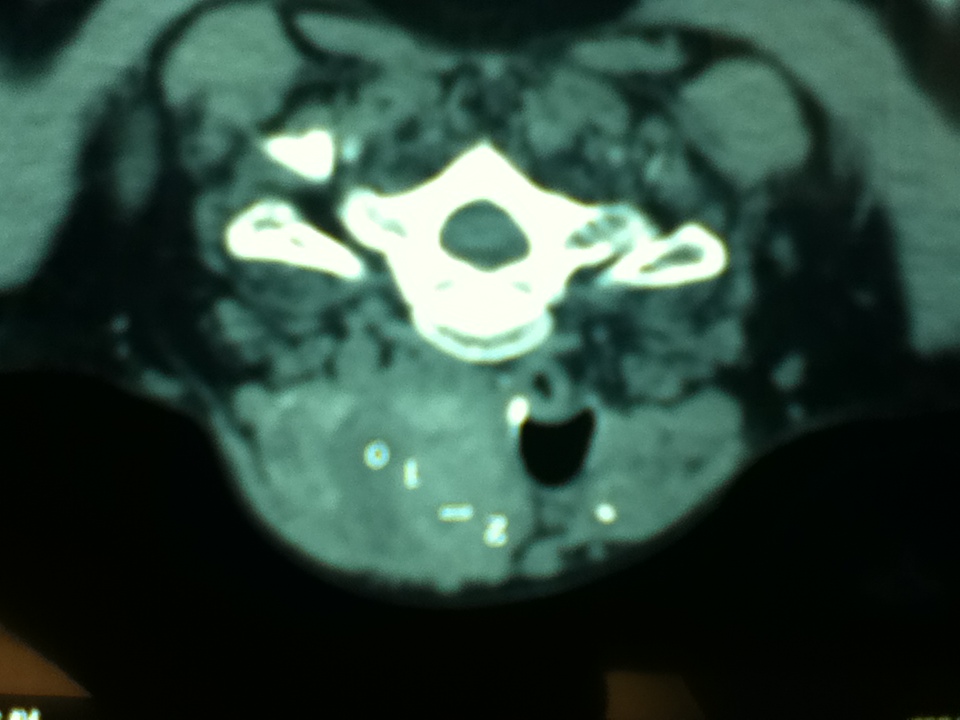
QUESTION--I am an endocrinologist from Mexico. This is the neck CT (see below) of a 65 year old woman who consulted because a muscular complaint in the upper back. She had a modest goiter and no other symptoms. Her TSH was 3.6. T3 and T4 normal. No antibodies. No respiratory complaints. The patient refused surgery. My question is: what treatment option does the expert suggest in this patient? Jose Diaz Suare, MD
RESPONSE--Thank you for asking us to suggest the best treatment for your patient, a 65 year old female with a moderate goiter and normal thyroid functions. As the patient did not agree to be submitted to a surgical procedure, the best treatment could be the use of recombinant human thyrotropin (available in the US) followed by radioiodine treatment. Two recently published studies are indicated below:
Fast S, et al. Long-term efficacy of modified-release recombinant human thyrotropin augmented radioiodine therapy for benign multinodular goiter: results from a multicenter, international, randomized, placebo-controlled, dose-selection study. Thyroid. 2014 , 24(4):727-35. doi: 10.1089/thy. 2013.0370. Epub 2014.
Graf H. Recombinant human TSH and radioactive iodine therapy in the management of benign multinodular goiter. Eur J Endocrinol. 2015, 172(2):R47-52. doi: 10.1530/EJE-14-0608. Epub 2014. Review.
Sincerely, Geraldo Medeiros-Neto, MD
HYPOTHYROID SYMPTOMS (?) AND THEIR TREATMENT- 3 September 2014
QUESTION-I will appreciate for help in another patient who is a neurosurgeon, had RAI for graves disease in 2009. He has been on levothyroxine since then but for last 6-8 months, he has been having episodes of dizziness and vertigo. He tend to have these symptoms when his TFT levels are in euthyroid range but feels extremely WELL when his TSH is high. His TFT are shown below. I checked his TSH with HAMA and it did not change. As you can see, in May 2014, when his TFT were normal, we had to admit him to hospital for his symptoms. His alpha subunit to TSH ratio is less than 1 when his TSH is 5.5 FT4 is 1.1 ad FT3 is 2.0 and alpha subunit is 0.5. MRI of pituitary has been done and is normal.
Is it pituitary resistance to TH that he AQUIRED in 2013?
Iftikhar A. Malik, M.D. , TCP Endocrinology
| Component | FREE T3 | T4 THYROXINE, FREE | TSH |
| Latest Ref Rng | 2.8-5.3 pg/mL | 0.7-1.9 ng/dL | 0.50-5.00 uIU/mL |
| 3/7/2011 | 3.4 | 1.3 | 3.12 |
| 9/2/2011 | 3.2 | 1.5 | 3.99 |
| 1/6/2012 | 3.6 | 1.3 | 4.22 |
| 2/18/2013 | 3.2 | 1.3 | 4.42 |
| 7/17/2013 | 3.7 | 1.6 | 2.15 |
| 10/8/2013 | 4.17 | ||
| 12/23/2013 | 7.81 (H) | ||
| 2/7/2014 | 10.60 (H) | ||
| 3/25/2014 | 8.05 (H) | ||
| 4/25/2014 | 3.3 | 0.8 | 9.11 (H) |
| 5/18/2014 | 3.1 | 1.8 | 1.18 |
| 5/27/2014 | 3.0 | 1.1 | 12.30 (H) |
| 6/6/2014 | 3.0 | 0.9 | 14.20 (H) |
| 6/28/2014 | 2.8 | 0.8 | 17.60 (H) |
| 7/31/2014 | 3.0 | 1.0 | 19.20 (H) |
| 8/26/2014 | 3.1 | 1.3 | 12.57 (H) |
RESPONSE-Whether the episodes of dizziness and vertigo related directly to the thyroid hormone levels in the past is unclear. but they could at this time. Most likely your patient needs a slight increase in T4 dose. Most patients on thyroxine need to have a T4 at the top end of the normal range in order to be properly replaced, with normal T3, TSH of 1-2, and feeling best (as on 5/18). The TSH recorded on 5/18 is strange, but possibly his dose of thyroxine was somehow higher just before that test, since his fT4 was at the unusual level of 1.8 at that time. L De Groot, MD
ADEQUATE IODINE SUPPLEMENTATION IN INDIA?? 22 July 2012
QUESTION-Currently, in India we are consuming iodized salts everyday still there is very high prevalence of thyroid cases. My question is that in clinical practice do doctors need to completely avoid any nutritional supplement containing iodine (100-150mcg), considering that we all are consuming iodine salts and additional iodine containing preparation though in nutritional amount will be harmful to patient. Kindly throw some light on this issue. Makwana Altaf A; M.Pharmacy (Pharmacology)
RESPONSE-As you have correctly pointed out the Universal Salt Iodisation Program (USI) in India has had its “ups and downs” and there have been many reports in the literature of it not being as effective as one had hoped for.
Indeed, in a very recent publication in Clinical Endocrinology by Marwaha et al ( Vol 76,905-910) it is clear that iodine deficiency remains prominent in India. In the study population of schoolchildren in Delhi 16.4% had goitre and 7.3% were hypothyroid.
If you cannot access the article please let me know and I will send it to you.
Dr Pandav from AAIMS informs me that current iodised salt coverage in India is only 71%, therefore one would expect to see persistence of endemic goitre and other manifestations of IDD.
The current WHO/ICCIDD/UNICEF recommendation is that where USI coverage is not effective then pregnant women should be taking an iodine supplement of 150 ug per day. There is no recommendation for men or children to take a supplement. It is recommended that iodine intake should not exceed 500 ug per day. The normal iodine RDI for adults and children is 150 ug and for pregnant and breastfeeding women it should be 250 ug per day.
Sincerely, Prof C J Eastman AM